Athlete of the Month
How our sports rehab in Smithtown for an adductor strain helped our athlete return to the soccer field!
HIP TERMS:
Hip abduction – the act of bringing leg away from the body
Hip adduction – the act of bringing leg towards the other leg
Concentric strength – actively contracting/shortening the muscle of interest
Eccentric strength – strength required to control the opposite motion of muscle of interest
- For example – biceps
-
-
- Concentric = actively flexing elbow
- Eccentric = controlling elbow extension
-
Isometric strengthening – a type of strengthening that does not involve an active movement of the muscle contracted. For example, squeezing a ball between your legs is considered a hip adductor isometric.
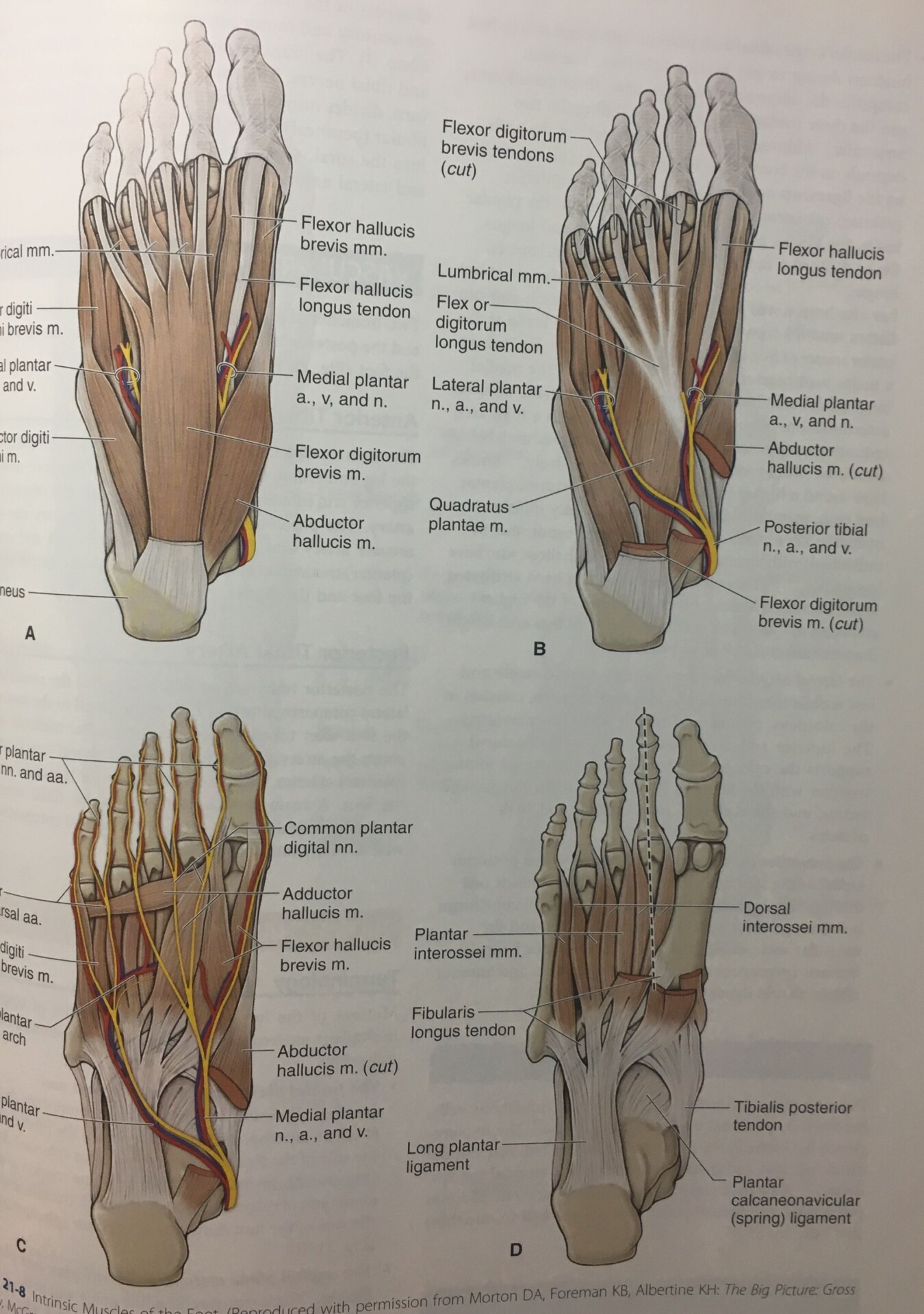
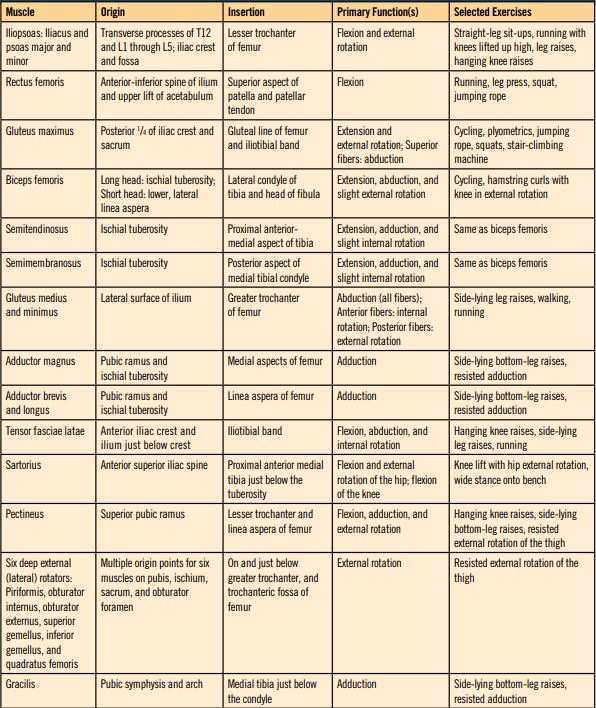
HIP ANATOMY AND MUSCLE ACTIONS:
Anatomy


OUR ATHLETE:
Madison: 13-year-old soccer player
History:
Madison arrived at Block Chiropractic Sports and Physical Therapy in Smithtown, NY after suffering a hip injury while playing soccer. Initially, she was evaluated by our chiropractor and later that week she was referred to our physical therapist for further examination. She walked through the front door the day of her evaluation hesitant and nervous since she has not experienced a sideline injury before.
Injury:
Madison states while playing soccer, she went in for a slide tackle and hit the ball and defender at the same time. Upon contact, she felt instant pain in the inside of her right thigh. She continued to play the game and felt increasing pain as the game went on. She attempted to rehab and ice herself for the next three weeks, however, she reported that there was no change in symptoms.
Subjective complaints:
The pain was rated 1-2/10 at rest but 8-9/10 with activity (on a subjective 0-10 scale with 0 being no pain and 10 being the most severe pain). Activities that worsened pain included: walking, going up/down stairs, running, squatting, lunging and playing soccer.
In clinic evaluations:
Chiropractic exam:
Upon evaluation by our chiropractor in Smithtown who has experience in sports injuries, Madison was found to have the following impairments:
-
- Tightness in bilateral hip flexors (psoas muscles)
-
- Tightness in bilateral hip external rotators (piriformis muscle)
-
- Tenderness to right rectus femoris (major quadriceps muscle that crosses both hip and knee joints), right adductor magnus, longus and brevis (hip adductors) and bilateral piriformis muscles
-
- Trigger points (“knots”) in RIGHT rectus femoris, RIGHT adductor longus, BILATERAL piriformis
- (+) Special tests for thigh tightness (Yeoman’s test) and hip impingement (FABER or Patrick’s test)
Physical therapy exam:
In addition to chiropractic findings, other areas of Madison’s lower body joints, musculature and functional mobility were tested by our physical therapist in Smithtown.
-
-
- Pelvic alignment: Madison was found to have an Anterior Pelvic Tilt (APT) on her right side.
- Explanation – This means that the front side of her right pelvis was rotated forward compared to her left side. This can cause abnormal mechanics during walking, running, squatting and lunging that are contributing to her pain.
- Pelvic alignment: Madison was found to have an Anterior Pelvic Tilt (APT) on her right side.
-
- Standing posture: While analyzing the way Madison is aligned while standing, she was found to have hip abductor weakness, hip flexor tightness, gluteal weakness and abdominal weakness.
- Explanation – Normally, we would like your hips level from side-to-side and front-to-back. However, when weakness occurs, this can be altered (similar to explanation during pelvic alignment).
-
- A common postural dysfunction of the lower body is called Janda lower crossed syndrome. With this, the front half of the pelvis is shifted forward and downward compared to the back. In theory, this means that hip flexors and back extensors are commonly tight while hip extensors (glutes) and abdominal muscles are weak.
- Another common postural impairment is called Trendelenburg. With this, when standing on one leg, the opposite hip will drop inward insinuating hip abductor weakness.
-
- Explanation – Normally, we would like your hips level from side-to-side and front-to-back. However, when weakness occurs, this can be altered (similar to explanation during pelvic alignment).
- Standing posture: While analyzing the way Madison is aligned while standing, she was found to have hip abductor weakness, hip flexor tightness, gluteal weakness and abdominal weakness.
-
- Hip joint mobility: While testing Madison’s right hip, she was found to have a decreased lateral glide.
- Explanation – In order for the hip to move correctly, the head of the femur (ball) must glide in the acetabulum (socket). For example, in order to achieve hip flexion and internal rotation, the femur must glide posteriorly (backward) in the socket. To extend and/or externally rotate the hip, the femur must move anteriorly (forward) in the socket. Distraction (the act of pulling hip toward feet) and lateral glide (bringing femur outward), allow for anterior and posterior glides to happen correctly. Therefore, by improving LATERAL glide in Madison, her hip will be able to move through her range of motion better causing less pain and stress on hip structures.
- Hip joint mobility: While testing Madison’s right hip, she was found to have a decreased lateral glide.
-
- Hip range of motion (ROM): Madison was found to have decreased pain-free hip flexion, extension, adduction, abduction, internal rotation and external rotation in her right hip. Values were normal in the left hip.
- Explanation – There are certain normal values for ROM of the hip. See below for Madison’s findings compared to normal values found in Dutton’s Orthopedic Examination, Evaluation and Intervention textbook. (Madison/Normal range).
-
- Hip flexion – 59/110-20
-
- Hip extension – 8/10-15
-
- Adduction – 7/25-30
-
- Abduction – 15/30-50
-
- Internal rotation – 23/30-40
- External rotation – 39/40-50
-
- Explanation – There are certain normal values for ROM of the hip. See below for Madison’s findings compared to normal values found in Dutton’s Orthopedic Examination, Evaluation and Intervention textbook. (Madison/Normal range).
- Hip range of motion (ROM): Madison was found to have decreased pain-free hip flexion, extension, adduction, abduction, internal rotation and external rotation in her right hip. Values were normal in the left hip.
-
- Hip strength (MMT): Madison was found to have a good isolated strength of left hip musculature, but was found to have significant weakness in right hip flexion, extension, adduction, abduction, internal rotation and external rotation. Greatest weakness was in the flexion and adduction. The pain was also present during testing of these two motions.
- Explanation – Isolated muscle strength is typically graded by a manual muscle test (MMT). The highest/strongest grade is considered 5 and the lowest/weakest grade is considered a 0. Within each number grade, there can be a (+) or (-) grade, meaning slightly stronger or weaker, respectively. See below for specific muscle strength of both hips.
-
- Hip flexion – Right = 3-/5, Left = 5/5
-
- Hip extension – Right = 4-/5, Left = 5/5
-
- Hip adduction – Right = 3-/5, Left = 5/5
-
- Hip abduction – Right = 4-/5, Left = 5/5
-
- Hip internal rotation – Right = 4-/5, Left = 5/5
- Hip external rotation – Right = 4-/5, Left = 5/5
-
- Explanation – Isolated muscle strength is typically graded by a manual muscle test (MMT). The highest/strongest grade is considered 5 and the lowest/weakest grade is considered a 0. Within each number grade, there can be a (+) or (-) grade, meaning slightly stronger or weaker, respectively. See below for specific muscle strength of both hips.
- Hip strength (MMT): Madison was found to have a good isolated strength of left hip musculature, but was found to have significant weakness in right hip flexion, extension, adduction, abduction, internal rotation and external rotation. Greatest weakness was in the flexion and adduction. The pain was also present during testing of these two motions.
- Functional Movement Screen (FMS): The FMS is a test that puts the athlete through a series of 7 functional movements – (1) squat, (2) stepping, (3) lunge, (4) reaching, (5) leg raising, (6) push-up, and (7) rotary stability. Each movement is graded on a scale of 0-3 with 3 being perfect form and 0 being unable to perform or pain with movement. Throughout each movement, certain ROM and functional strength deficits can be identified. Madison was exposed to tests 1-3, 5 and 7 and was found to have functional weakness in glutes, hip abductors and ankles, decreased functional mobility of ankle and thoracic spine and instability in bilateral ankles and hips.
-
- Explanation – In order to perform the 7 motions listed above, proper functional ROM and strength are required. Click here for test procedures and grading criteria.
- (+) Special tests for: Hip impingement (scour’s test), iliotibial band (ITB) tightness (Ober’s test), hip flexor and quad tightness (Thomas test) and hamstring tightness (90/90 test).
Diagnosis:
Upon collaboration between our chiropractor and physical therapist at our sports rehab in Smithtown, Madison was diagnosed with a grade II adductor, or “groin,” strain. On top of her muscular injury, she was found to have decreased joint mobility of the right hip, muscle imbalances of the core and hips and instability in her ankles and hips. With these impairments, Madison was left susceptible to muscle strain.
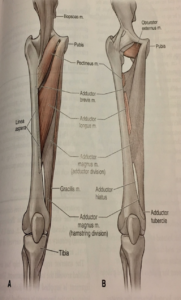
“Groin” definition, function and how it can be injured:
Many people refer to the muscle group on the inside of their thigh as the “groin.” The groin is actually composed of six muscles that work together to bring the leg toward the other (adduction). These muscles are also responsible for controlling the hip moving away from the other (abduction). This act of controlling the opposite motion is known as eccentric strength. It is the lack of this eccentric strength that contributes greatly to groin injuries. The six muscles are as follows: 1) adductor longus, 2) adductor magnus, 3) adductor brevis, 4) pectineus, 5) gracilis and 6) obturator externus (when the hip is flexed).
Here at Block Chiropractic Sports and Physical Therapy, we have provided rehabilitation for groin injuries in Smithtown to several of our athletes. Our experts in sports rehab in Smithtown, know that groin injuries are a very common sports injury, especially for soccer players. During running and sprinting, the adductor muscles are one of the most common muscles called into action. They are recruited during 25% of the running cycle and are responsible for providing support during stance phase and accelerating the leg back forward to begin swing phase. When muscle imbalances like Madison’s occur, the adductors are A) forced to try and compensate for surrounding weak muscles and B) are not strong enough to control the quick movements of the leg. With this, the muscles become irritated and can become strained, leaving the athlete in significant pain and discomfort.
Muscle strain definition:
Muscle strains can be broken down into three levels and are described as follows:
-
- Grade I – is defined as the mildest muscle injury out of the three. It is referred to as an overstretching of the muscle and its fibers. Clinically, the patient has minimal pain that is localized to the area of injury, mild-to-no disability and full to nearly-full (less than 10-degree deficit) ROM. With this injury, the athlete typically returns to athletic competition within 0-2 weeks.
-
- Grade II – is defined as a “moderate” injury. With this grade, the muscle can have mild tears of the fibers. This can range from barely torn to severely torn, however, it is not completely ruptured. As you can guess, this has a wide range of presentation. More often than not, the patient will report moderate diffuse pain, moderate disability during sport, greater ROM deficits (10-25-degree deficit) and possible bruising. Grade II strains can leave the athlete out anywhere from 2-8 weeks.
- Grade III – is considered a full tear of the muscle, leaving the athlete completely unable to play the sport and possible everyday activities. The patient often reports severe diffuse pain, significant bruising and swelling, decreased ROM (greater than 25 degrees) and decreased strength. This injury is typically traumatic and requires immediate removal from athletic competition. Grade III strains can leave an athlete out of competition for 8-12 weeks, if not more.
Risk factors for groin injury:
-
- Hip abductor weakness (+ Trendelenburg)
-
- Decreased hip adductor concentric and eccentric strength
-
- Decreased hip abductor ROM/groin tightness
-
- Poor training
-
- Return to competition too soon after injury
- Previous leg injury or previous groin strain
Rehabilitation:
At Block Chiropractic Sports and Physical Therapy, our chiropractor and physical therapist for sports rehab in Smithtown and Selden are well trained in treating the high-level athlete with a pulled groin, or adductor strain. Rehabilitation for this injury is based off the level, or grade, of strain. In our sports rehab in Smithtown and Selden, we do not solely treat the groin strain, but also the impairments and dysfunctions that caused the athlete to be susceptible to the injury in the first place.
Mild and moderate strains are typically treated conservatively with good success. During the first 24-48 hours, it is believed that ice and compression can help decrease pain and muscle spasm. After 24-48 hours, ice does not have the same benefits, however, it can continue to help decrease pain naturally while avoiding prescription medications. Also during this time frame, it is beneficial to begin light intervention. Light intervention can include gentle soft tissue massage, gentle joint mobilizations, muscle energy techniques (METs), submaximal isometrics to adductors, strengthening of weak hip muscles, hip pain-free passive ROM, flexibility training of non involved muscles, core strengthening in pain-free positions, double leg balance exercises and modalities as needed.
After 7-10 days, or when active adduction is no longer painful, the patient at our sports rehab in Smithtown can progress to the sub-acute phase. This consists of the progression of strengthening and ROM exercises from phase I while continuing modalities and manual therapies. At this time, the athlete may begin functional training and add higher level pain-free exercises. Some exercises include (but are not limited to): squats, straight leg raises emphasizing adduction, single leg balance, hip abductor strengthening, flexibility of lower extremity muscles, planks, and side planks.
At approximately the 4-6-week mark, depending on the severity of the injury, the functional and sports-specific training at our sports rehab in Smithtown or Selden can begin. In order to progress to this phase, the athlete must have full pain-free ROM in all directions and have at least 80% strength of the opposite limb. This is the fun phase! The athlete can begin sports-specific drills involving agility and speed work, higher resistance training and dynamic core and balance training. The patient may then be discharged from our sports rehab in Smithtown or Selden when the strength of injured limb is 90-100% that of opposite leg.
Return-to-sport protocol:
At Block Chiropractic Sports and Physical Therapy, our doctors for sports rehab in Smithtown use a return-to-sport protocol to determine if the athlete can safely return to athletic competition. Our return-to-sport protocol consists of:
-
- Single leg hop for distance
-
- Single leg triple hop test for distance
-
- Single leg crossover hop for distance
-
- Jump downs/landing (looking for proper eccentric control and form)
-
- Repeated FMS screen
- Sports-specific skills (for example: kicking, carioca’s, agility ladder)
They are cleared when results of the injured leg are 80% of the healthy leg. When they clear this test, it does not mean they should be discharged, as there are likely impairments and weaknesses that will remain. It allows them to begin the transition back to sport under supervised care to best prevent re-injury.
Madison’s program:
To return to our athlete of the month! Madison worked very hard for approximately 7 weeks. She was treated by our chiropractor and physical therapist in our sports rehab in Smithtown for her groin injury. The early phase of treatment consisted of Active Release Techniques (ART), manual stretching and lumbopelvic manipulation from a chiropractor. ART is a form of soft tissue mobilization that consists of pinning a trigger point found in a muscle and have the patient actively stretch that same muscle. Manipulation was based on the results from our sports rehab in Smithtown. Our chiropractor completed a skilled examination to determine which joints may require improved mobility. Simultaneously, physical therapy provided in our sports rehab in Smithtown consisted of early joint mobilization of the hip, soft tissue massage to the thigh and low back, METs to correct pelvic alignment and low-level exercise was initiated. Light exercise consisted of adductor isometrics at 25-50% strength, pain-free stationary bike, pain-free core exercises, pain-free hip abductor strengthening, and stretching of the hamstring, hip flexor, and quadriceps.
As Madison achieved pain-free hip adduction during exercise, her exercises were progressed. She continued with higher level core and single leg balance exercises, began adductor strengthening through the entire range, and implemented dynamic stabilization exercises such as monster walks, physio ball squats, hip hiking, bridges, and RDLs. Manual therapies progressed to involve Instrument Assisted Soft Tissue Mobilization (IASTM) that uses a safe metal tool that allows the provider to reach deeper tissues to break up adhesions and restrictions. Other manual therapies by our doctors at our sports rehab in Smithtown were continued. Manual proprioceptive intervention, known as PNF exercises, were also implemented to begin retraining more efficient movements.
Madison finally reached pain-free dynamic activity between weeks 5 and 6 of her program. She was put through the testing in our return-to-sport protocol and passed. However, she felt mild discomfort during carioca exercise. She was allowed to return to predicted, contact-free soccer activities with a focus on skill work for 1 week. After 1 week, she was retested and was pain-free in all exercise.
The shy, apprehensive athlete that walked in our door 7 weeks prior happily returned to full soccer competition and reported pain-free competition. She is playing on an elite travel soccer team that travels several times a year to play in competitive tournaments and is currently training with her high school varsity team, as well. Madison was very compliant with her home exercise program and resting from competition and because of that, had great success at Block Chiropractic Sports and Physical Therapy in recovering from her groin strain.
How to prevent an adductor strain:
Most adductor strains can be prevented with a good training program. Programs should consist of core strengthening, hip abduction strengthening, balance and proprioceptive exercises, flexibility work and functional mobility training. Many training programs consist of only strengthening big muscle groups, however, it is important to include functional mobility training. If the joint is not moving through its full ROM, muscles work inefficiently and are prone to injury.
How we can help you!
Our doctors at our sports rehab centers in Smithtown and Selden are highly experienced in treating groin strains. Our chiropractor in Smithtown is certified in ART. In addition, the chiropractors at our clinic are head chiropractors for local collegiate athletic teams. College teams that are under our care include Stony Brook University, Queens College, and Long Island University Post. Additionally, we treated the NY Cosmos, a semi-professional soccer team for several years.
The physical therapists in our clinics are all Division I athletes who have experienced muscle strains themselves. At our sports rehab center in Smithtown, our physical therapist can relate to the injured athlete and understand the dedication to return to competition. Additionally, we have physical therapists trained in Graston® Technique, a type of IASTM, and Selective Functional Movement Assessment (SFMA) which is a high-level screen to find mobility and strength deficits of several joints that may be hindering athletic performance. We incorporate the FMS screen into evaluations for the majority of our athletes who come into the clinic. We are proud to say that we have had high success in rehabbing groin injuries in Smithtown and Selden.



{kind=link}