What Is The SFMA?
The Selective Functional Movement Assessment, or SFMA, is a screening tool developed by Lee Burton, Gray Cook, Kyle Kiesel and Greg Rose that allows a practitioner to find mobility and stability deficits in patients. Mobility refers to a joint range of motion (ROM) that may be limited due to joint restriction or soft tissue tightness. Stability refers to motor control, which is the body’s way of controlling and coordinating movement through specific patterns. Dysfunctions in motor control can be caused by impairments such as decreased strength, decreased proprioception (body’s position in space), decreased coordination and many more. The SFMA is a comprehensive assessment that breaks down 10 functional movement patterns to determine the location of these dysfunctions. By finding these hidden impairments, the practitioner can create a better plan of care to best heal their patient. We have SFMA providers for physical therapy in Selden and Smithtown, NY who would love to educate you more on how the SFMA can benefit you.
SFMA’s key concepts:
The SFMA was created based off of key concepts the founders felt were often overlooked when diagnosing patients. Below, we will outline the main ideas of these key concepts:
- Regional interdependence – “the concept that seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint.” In simpler terms, it explains the concept that all body parts are connected and as a result, the location of pain is not often where the source of the pain is. That is, a patient may have pain in the low back, but the reason the low back hurts is because the hip is not moving well. The silly song they teach kids where they sing “the hip bone’s connected the backbone” is very true. This idea of regional interdependence is important when determining the plan of care for the patient. If we simply treat the location of pain, we will most likely decrease the pain, however, we are not solving the problem. Therefore, the pain will likely return when high demands are reinstated.
- Mobility and stability alternating patterns – “The body works in an alternating pattern of stable segments connected by mobile joints.” To help understand this, joints are designed to function for stability or mobility. Stable joints are typically stronger and are built for support rather than range of motion. On the other hand, mobile joints are built to move differently to achieve greater ranges of motion. The body is essentially a stack of alternating stable and mobile joints (see list below). This is great in theory until a joint does not function properly and causes the connecting joints to have to overcompensate. When you lose mobility in one joint, the stable joint connected to it tries to gain movement. However, the stable joint is not built to do so. When this happens, that stable joint becomes irritated and pain can occur. Without an SFMA, the provider may target this painful joint and neglect the hypomobile joint that is really the source or cause of the pain. An SFMA provider will properly screen movements to find this hidden mobility issue to hopefully prevent future recurrence of pain.
If you have any questions or need further clarification about these key concepts, contact our physical therapy in Selden and Smithtown.
List of joint patterns (from bottom->top)
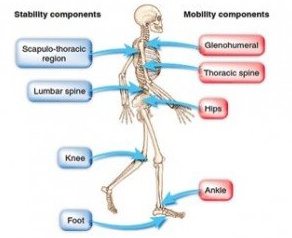
Foot – stable
Ankle – mobile
Knee – stable
Hip – mobile
Lumbar spine/pelvis – stable
Thoracic spine – mobile
Scapula-thoracic – stable
Shoulder – mobile
Elbow – stable
Wrist – mobile
Cervical spine – stable
PATIENT EXAMPLE – A patient arrives with low back pain. The lumbar spine is built as a stable joint, meaning it is not designed to move a significant amount. Upon further examination at our physical therapy in Smithtown and Selden, the hip (a mobile joint) is found to have a decreased range of motion. Because the hip is not moving well, the low back is trying to overcompensate and gain the missing range of motion. However, because it is not built for this, it becomes overworked and irritated. This is how pain begins.
- Pain and motor control – As explained above, motor control is the idea that the body has systems in place to control and coordinate movement through certain patterns. However, when we have an injury that causes pain, the body moves differently. The body does not want the painful muscle or action to be called upon and will, therefore, alter the way it moves to protect itself. When this compensation lasts too long, the long-term consequence is a dysfunctional movement that will put stress on an adjacent or related body part. This can then lead to increased pain or injury in a new area, causing two problems now instead of one. An example of this is when someone sprains their ankle. They compensate by limping and shifting weight to the opposite leg. The longer this person limps though, stress is now added to the opposite hip and now their hip begins to hurt. This can be especially problematic in athletics when an athlete is playing through an injury and altering the way they are moving. This can often lead to changed running or landing mechanics which can, in turn, lead to ACL tears or lumbar disc herniation.
- Movement pattern vs. isolated movement – The body is built to move as a unit to accomplish basic movement patterns. How often do you simply flex only your elbow (bicep curl) during the day? Rarely. However, you move your elbow when you reach above into a cabinet to grab something. Often times, we only look at an isolated joint and its range of motion. We need to look more at the body as a whole, moving through movement PATTERNS. This is a more functional approach and will allow us to determine whether the joint is able to help perform the task at hand. To outline the importance of this concept, we will look at your core. A male patient arrives to our physical therapy in Selden and Smithtown offices with a six-pack of abs and states he does a lot of sit-ups. His biggest complaint is low back pain. If we test only the strength of his core, he may appear to very strong and we may not think he needs training in this area. However, when we test his movement pattern, such as an overhead squat, he is unable to maintain balance and proper back positioning through the motion. Therefore, he has good isolated strength of the core but poor FUNCTIONAL strength of core which is likely contributing to his low back pain.
- Neurodevelopmental perspective – This concept refers to the order in which we learn movement from the day we are born. The normal sequence in which we learn how to move is:
Breathing → grasping → head/eye movement → limb movement → rolling → crawling → kneeling → transitional movements → standing
The SFMA uses this pattern of learning to create a plan of care. We retrain your strength and motion in the most basic patterns first. Once we re-master the simpler movements, our physical therapy in Smithtown and Selden progresses to higher level functioning.
SFMA for physical therapy in Selden and Smithtown tier movements and breakouts:
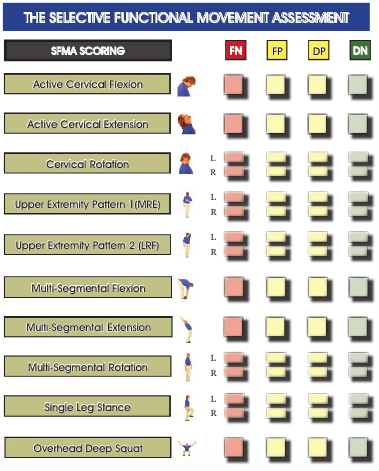
The SFMA begins by screening 10 “tiers.” These include:
-
- Cervical flexion
-
- Cervical extension
-
- Cervical rotation
-
- Upper extremity pattern 1 (medial rotation + extension [MRE])
-
- Upper extremity pattern 2 (lateral rotation + flexion [LRF])
-
- Multi-segmental flexion
-
- Multi-segmental extension
-
- Multi-segmental rotation
-
- Single-leg stance
- Overhead deep squat
These tiers are classified in 1 of 4 categories:
-
- Functional Nonpainful (FN)– moves correctly, pain-free
-
- Functional Painful (FP) – moves correctly, experiences pain
-
- Dysfunctional Painful (DP) – moves incorrectly, experience pain
- Dysfunctional Nonpainful (DN) – moves incorrectly, pain-free
Of course, if the movement pattern is FN, we leave it alone! It is working correctly and not causing the patient any pain. For movements classified as FP and DP, during physical therapy in Smithtown and Selden, we break down these patterns with caution, since pain is present. Movements found to be DN are also broken down further to determine where dysfunction is coming from. Pain is treated first and once the pain is gone, the underlying mobility or stability deficits will be addressed.
For the sake of time, I will outline quickly how the breakdowns occur. However, I am not going to explain each and every breakout for all 10 tiers.
The breakout section is a flowchart used to break down each of the 10 tiers. They consist of the basic joint movements required for each movement pattern. For example, the break out of MRE will include shoulder, elbow and thoracic movement, because all 3 of these are required to complete that pattern. First, the movement is performed in an anti-gravity position to eliminate postural demands. If a movement is now functional in this gravity-eliminated position, the breakdown is typically done and it is likely that the patient has a stability dysfunction. Meaning that the body CAN perform the movement at task, however, IT DOESN’T KNOW HOW TO. If the movement remains dysfunctional, then the examiner will now bring them through that movement passively. If the movement is functional at this time, then again, it is likely a stability issue. However, if the movement remains dysfunctional, we break down the movement, even more, to determine where the dysfunction lies. To go back to the MRE example, we now look at those 3 motions. More often than not, if we have reached this point, mobility deficits are being found. Meaning that the range of motion is not there to complete the task. Below is an image of the MRE breakout :
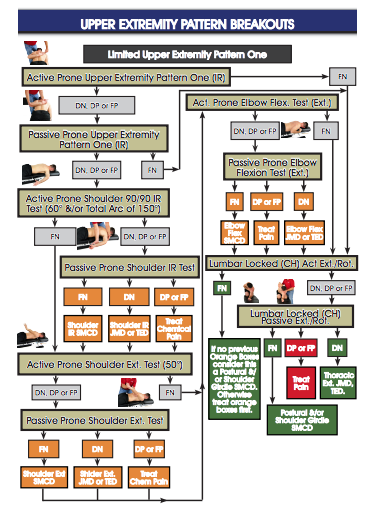
From here, we have a diagnosis of mobility or stability dysfunction. When our physical therapists in Selden and Smithtown reach a mobility dysfunction diagnosis, we must now do a thorough examination of the joint to determine if it is joint hypomobility or soft tissue restrictions causing the lack of motion. This is beyond the scope of the SFMA, but the SFMA helps determine which joints to dive deeper into to help determine ideal plan or care. When the SFMA is complete, the examiner will have a list of diagnoses. The plan of care typically begins superiorly, and mobility deficits will be addressed first. Why train movement when movement is not being achieved?
SFMA for physical therapy in Smithtown and Selden treatment plan :
-
-
- Mobility -> stability
- SFMA authors suggest treating mobility deficits prior to working on stability. This is because if you are providing strength to an abnormal or limited movement, you are reiterating the dysfunction. Therefore, it is important to correct the movement issue so that the patient is able to move with proper range. It is after this is achieved, that we add strengthening to the now corrected movement.
- Mobility -> stability
-
- The general guidelines of the SFMA treatment protocol for physical therapy in Selden and Smithtown can be referred to as the “Three R’s.”
- Reset – Reset is mostly in the hands of the practitioner. It is recommended that providers used manual intervention to improve the mobility or stability dysfunction. Interventions may include joint mobilizations, manipulation, myofascial release, Active Release Treatment (ART), Graston Techniques and more. These should be techniques implemented by PROVIDER, rather than simply providing exercises to the patient.
-
-
-
- Re-enforce (reinforce) – It is our job as practitioners to provide the patients with modalities and education to prevent relapse into old, poor movements. We may use interventions such as orthotics or kinesiotape to enforce improved posture and movement patterns. However, it is also important for use to master our words and supply the patient with the knowledge of contraindications and activities to avoid until the next treatment session. This will reinforce the corrections made with our “reset” techniques.
- Reload – This is when we begin implementing corrective exercises during newly acquired ranges and form. It is recommended by SFMA for physical therapy in Smithtown and Selden to focus primarily on the dysfunctional non-painful patterns. To begin adding in exercises, the SFMA provides a 4-by-4 guideline, in which there are four types of positions and four types of resistance.
-
-
- Four by Four:
-
- Four Positions =
-
- Supported – typically prone (lying on stomach) or supine (lying on back) because there is minimal postural demands or gravity resistance.
-
- Suspended – quadruped (or “all fours”) position. This begins adding postural demands and mild gravity resistance.
-
- Stacked – half-kneeling. Again, this begins increasing demands and gravity.
- Standing
-
- Four Positions =
- Four Resistance Types:
-
- Feedback – providers supplying assistance
-
- Demonstrate – going through the motion with no help or resistance; simply using body weight and gravity.
-
- Capacity with Feedback – begin adding resistance to the movement while providers are able to supply assistance
- Capacity – add resistance with no help
-
-
How SFMA for physical therapy in Selden and Smithtown can help decrease pain:
The SFMA can help providers show patients where their pain is coming from. It is often hard to convince a patient with chronic low back pain that the source of pain isn’t their back. By putting them through the SFMA, it allows them to see first hand their deficits through certain activities and motions they perform every day. Because of this, the providers at our physical therapy in Smithtown and Selden are able to hone in on the cause of their pain. To use the same example of low back pain, the practitioner can now work on the thoracic spine and/or hip mobility to decrease the stress put on the low back during a squat. By decreasing the stress, the low back is able to subsequently work and move better and pain will, in turn, be decreased. The SFMA allows us to determine the root of the issue, rather than simply treating what we see and masking the true problem.
SFMA Can Improve Athletic Performance:
As explained above, the SFMA for physical therapy in Selden and Smithtown will bring to light important mobility and stability deficits. Athletic competition and training is demanding, and if the athlete does not have a proper range of motion or necessary stability to work through those demands, they may have increased pain or decreased peak performance. Athletes and coaches are highly knowledgeable about form, techniques, and mindset for their athletic competition, however, they do not necessarily understand what movement is required from specific joints to achieve these. For example, a baseball pitching coach understands the phases of throwing and proper weight shift. However, he may not fully understand that you also require scapula-thoracic stability, thoracic extension, bilateral hip rotation (opposite of throwing arm is most important) and proper rotational strength to healthily achieve this. Another example is with a cornerback in football where they have to make quick turns to adjust to a wide receiver trying to outrun them for a thrown football. Agility training can certainly make their feet faster, however, these athletes can become EVEN FASTER if they do not have to work extra hard to accomplish the same range of motion. While turning around to sprint, the athlete requires thoracic rotation, shoulder mobility, hip rotation, and ankle and core rotational stability.
Additionally, the SFMA for physical therapy in Smithtown and Selden can bring to light underlying dysfunctions that often lead to common injuries. For example, scapula-thoracic instability and decreased thoracic or hip rotation can put added stress on the medial elbow to complete the throwing motion. This added stress can leave the athlete susceptible to ulnar nerve injury or “Tommy John” symptoms. Contact our physical therapy in Selden and Smithtown to learn more about how SFMA can improve athletic performance.
Evidence-based support:
In a case report by Goshtigian and Swanson (2016), they explain how they used an SFMA to establish a treatment plan for an adolescent athlete with low back pain. The 18-year-old soccer player had a complaint of low back pain over the last 2 years. With the SFMA, it was determined that the patient had mobility limitations in the thoracic spine and both hips. After treating the low back first with soft tissue work to rid the severe pain, treatments to establish mobility throughout the thoracic spine and hips were implemented. They began first with manual intervention to “reset” the tissues and then supplied the athlete with proper corrective exercises to “reinforce” the changes. When the authors felt mobility was restored, they began “reloading” the tissues using exercises used throughout the patient’s typical exercise routine.
After 9 weeks of treatment with progression based off of SFMA recommendations, the patient was nearly functional, non-painful in every test, except right shoulder mobility. Additionally, he went from pain rated 2-7/10 to 0-2/10 at discharge. Therefore, using the SFMA to determine underlying impairments in this soccer player, helped target the probable cause of his low back pain and successfully decrease his pain.
In another case study by Kim and Yim (2016), they outline their evaluation and treatment plan for a recently pregnant woman with chronic patellofemoral pain syndrome (PFPS), a common knee disorder. The woman was 35-years-old with complaints of 8/10 knee pain. An SFMA revealed dysfunctional non-painful multi-segmental flexion and rotation (both ways), single leg stance (both legs), as well as dysfunctional painful multi-segmental extension and overhead deep squat. Additionally, she was limited by 8 degrees and 27 degrees in right and left hamstring length, respectively. Following a treatment plan to address tight leg musculature and corrective exercises using the four by four theory helped this woman decrease pain and improve mobility. After 8 weeks of guided rehabilitation, she reported 3/10 pain while gaining 8 degrees in the right hamstring and 18 degrees in left. With retest of the SFMA, she now demonstrated all functional non-painful movements, except multi-segmental rotation. Therefore, this study supports the idea that an SFMA can help determine an ideal plan of care and help relieve patients from pain.
How our physical therapy in Selden and Smithtown can help:
At Block Chiropractic Sports and Physical Therapy, we have three providers for physical therapy in Smithtown and Selden that are highly trained in SFMA evaluations. They have successfully utilized the SFMA in high school and collegiate athletes and helped them return to play better and faster. Whether you are or know an athlete, a weekend warrior, or someone with chronic pain, please stop by our Smithtown or Selden offices to schedule an SFMA. We will evaluate you and come up with a treatment plan and exercise routine to help correct your findings.



